
IESE Insight
Reforming healthcare for longer lives and better living

Aging populations demand we transform healthcare, building systems prepared to meet our societies’ demographic challenges.
By Nuria Mas
Ever longer lifespans combined with an increasingly older population is posing a serious twin challenge for industrialized societies around the world, especially those in Europe with welfare states providing universal healthcare.
For the first time in modern history, the number of people aged 50 and over is, in many cases, already outnumbering younger generations. This demographic shift upward holds major social and economic implications, requiring a profound rethink of the labor market as well as of healthcare policies, both in terms of how we provide care to others and how we would like to be cared for ourselves in our old age.
Preparing for this transition demands a deep understanding of the issues — and innovative thinking on how to tackle them.
A demographic shift with economic consequences
According to the EU’s 2024 Ageing Report (the latest year available, updated every three years), the share of those aged 65 and over went from representing 16% of the EU population in 2004 to 22% in 2024, with the share of those 80+ going from 3.8% to 6.1% over the same 20-year period. At the same time, birthrates are declining, resulting in a shrinking working-age population just as fiscal and care needs intensify.
This demographic shift is reflected in EU dependency ratios — the ratio of the old-age population to the working-age population. In 2022, for every 1 person over 65, there were 3 people of working age; by 2045, the projection is fewer than 2 workers for every person over 65.
The Ageing Report also notes that total age-related fiscal costs in the eurozone, measured as a share of GDP, will rise from 25.1% in 2022 to 29.1% by 2070. This higher expenditure will be entirely driven by healthcare and long-term care needs.
Meanwhile, countries are spending more on servicing their public debt than they are on healthcare or education. Global public debt hit a record $102 trillion in 2024, according to U.N. Trade and Development (UNCTAD).
Adding to countries’ fiscal pressures are unfunded future obligations like state pensions and long-term care commitments, with the ratio of social insurance entitlements to GDP ranging between 200% and 400% of annual GDP for 20 EU countries, and surpassing 500% in Spain. Although technically these expenditures do not register as debt, they constrain government budgets nonetheless.
With a significant share of working professionals due to retire over the next decade, the pressure is mounting for countries to redesign healthcare provision, as demand is going to reach unprecedented levels very soon.
Is more technology the answer?
Technological innovation, especially involving artificial intelligence (AI), is certainly going to play a pivotal role in what’s being called the Longevity Economy. The use of telemedicine has already become widespread since the COVID-19 pandemic, but we are also seeing the emergence of eldercare assistive robots — no longer the stuff of science fiction. That market is expected to exceed $10 billion by 2035.
Japan, which leads the world in having the highest ratio of people 65 and older, is earnestly developing humanoid robots to care for its burgeoning elderly population, given that there are simply not enough skilled workers to meet the demand. One Japanese care facility director said, “Technology is our best chance to avert” what he described as a “bleak” future.
Even so, these assistive robots lack social trust — a vital ingredient that the European Commission has said AI systems must fulfill, especially if they are being used in clinical settings. A 2024 study found that, while most EU citizens surveyed were open to using robots in healthcare, they were uncomfortable with letting robots make medical decisions over them or delegating triage to them; they also expressed strong concerns over the handling of sensitive personal data.
It’s a reminder that, even though technology offers promising solutions to our demographic challenges, it’s still not the sole answer.
The importance of professionalizing the care sector
Ultimately, high-quality care depends on the people who provide it: their training, working conditions and ability to build trust with those they support.
Professional care, however, remains undervalued. High turnover, low wages and limited recognition undermine continuity and quality. Research by IESE Prof. Marta Elvira shows that when caregivers receive proper training and opportunities for development and their work is valued, both their own wellbeing and that of their patients improve. Professionalization, clear career paths and stable working conditions are not luxuries — they are prerequisites for a sustainable care system.
A crucial piece of this puzzle is immigration. In many European countries, a significant share of care work is performed by migrant workers who play an indispensable role in residential facilities and home-care services. Yet another study by Elvira et al. reveals persistent pay gaps and integration barriers that limit these workers’ potential. In a context of growing labor shortages, failing to recognize — or enable — migrants’ contribution jeopardizes the system’s capacity to respond to the needs of an aging population.
The added challenge of chronic conditions in an aging population
As longevity increases, so will clinical complexity. More than 80% of primary-care users aged 45+ live with at least one chronic condition, and over half have two or more conditions, according to the OECD. The combination of aging and chronic disease raises an urgent question: how to deliver continuous care in healthcare systems designed for short, episodic interventions?
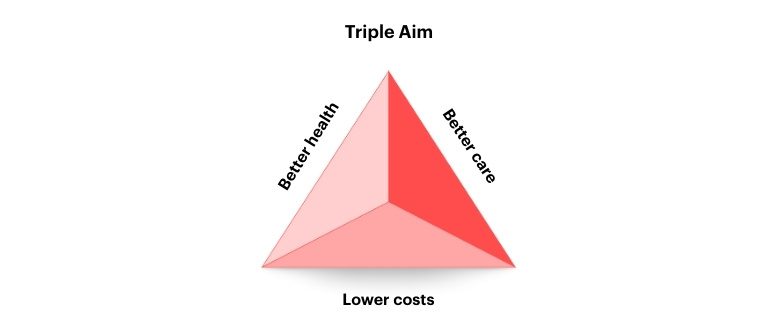
The Triple Aim
In my research on healthcare-system transformation, I argue we should be trying to achieve three objectives:
Better health
for the general population, which entails preventive care.
Better care
which means delivering the right care, at the right time and in the right place, thereby reducing complications and readmission rates. This, in turn, brings…
Lower costs
for both the treatment and the patient.
Improving the healthcare system requires not just delivering on any single one of these objectives, but rather delivering on all three of them simultaneously. That’s why I call this the Triple Aim.
To make progress toward the Triple Aim, we need to build on four operational pillars: data, patient-centered care, public-private partnerships and aligned incentives. To them I would add a fifth: developing care professionals. Together, these pillars yield the following practical recommendations.
5 recommendations for healthcare transformation
1. Use valid, shared indicators
Only 20% of the data needed to improve healthcare comes from within the system itself. The remaining 80% relates to lifestyle habits, the environment and socioeconomic factors — drivers of disease risk and prevention that often lie outside the clinical spotlight. At the same time, poor interoperability leads to duplication and errors.
Thus, it is important to gather the right data, but even more important is agreeing data standards and developing indicators that will be accepted by professionals and then shared across systems. Without common indicators, standardized measurement, shareable information and comparable results, improvement will be impossible.
2. Create legitimate, high-quality jobs in care
From the United States to Europe, there is a robust job market for healthcare practitioners and support occupations, with personal care aides and home health aides to assist the elderly being the fastest growing occupations, along with physical therapists and occupational therapy assistants.
A lot of these jobs depend on migrant workers, many of whom work in the informal labor market. As Elvira’s work underscores, formalizing and professionalizing these roles not only improves the quality of care but strengthens the labor market on which the system relies.
3. Align incentives to encourage better outcomes
Even the best systems fail when incentives are poorly designed. To illustrate: I recently studied what’s known as “dual practice,” whereby doctors split their time working in both the public and private sectors. My coauthors and I examined the efficacy of a Spanish policy offering bonuses to doctors to work exclusively in the public system. We demonstrated empirically that the bonuses backfired: doctors’ dedication to the public sector rose slightly, but the number of hours worked went down significantly; overall care did not improve and administration costs increased. In other words, offsetting bonuses were largely ineffective in achieving any of the Triple Aim objectives.
Incentives must be aligned to reward continuity of care, prevention and good clinical outcomes. Otherwise, efficiency will not improve, no matter how well-intentioned the idea behind the incentive.
4. Foster public-private collaboration
With public resources increasingly stretched, collaboration is indispensable, not to replace the public sector but to reinforce it. Intelligently designed public-service contracting can deliver proximity, innovation and excellence when guided by shared objectives and clear metrics. As with our study on dual practice, the issue is not to force a choice between public and private, but to ensure there are proper coordination mechanisms and incentive structures in place that reward value and results, no matter the choice.
This is important because the solutions will come not only through the public system but also through partnerships with third parties, especially tech providers. The medtech industry can help solve some of the problems related to continuity of care for elderly patients, who often suffer from the inefficiencies of a fragmented system by getting bounced back and forth between primary care centers, hospitals, public or private institutions specializing in patient recovery, home care providers and pharmacies.
5. Put the patient at the center
Person-centered care is not an aspiration — it is an operational requirement. Patients differ in needs and preferences; a one-size-fits-all approach cannot work.
Population stratification enables providers to identify clinical and social characteristics from the outset, ensuring that any professional involved understands the patient’s context. Care must then be adapted to individual preferences and engagement levels: Some patients want to be involved in every clinical decision; others prefer to delegate. Some value being treated at home; others feel safer in a hospital. Designing interventions that respect these differences reduces complications, improves adherence and eases anxiety for patients and families alike.
Integration works: a real-world example
One successful example of the Triple Aim in action occurred in a pilot in Catalonia for patients with complex chronic conditions. Regional healthcare and social care providers coordinated services in collaboration with patients and their families, based on these keys:
- Patient stratification. The first thing they did was codesign an individualized care and intervention plan based on the personal characteristics of the patient.
- Shareable electronic clinical records. This is the data piece. Every social worker, primary care doctor, specialist or emergency room doctor who saw that patient had access to the same information and kept adding more information to the system.
- A local agreement. Local needs were taken into account: a chronic patient requiring long-term care in a rural area is not the same as in the city. Once the main objective was agreed — to achieve the best possible healthcare outcomes for these complex chronic patients — then the local healthcare providers, both public and private, came together to decide how they would organize themselves to satisfy the needs of these patients.
The results were striking: readmissions after 30 days fell by 30%, and all quality indicators for chronic care improved.
This pilot demonstrated that the Triple Aim works when there is shared data, territorial coordination and a genuinely person-centered design.
The true dividend of longevity
We are facing a historic opportunity. The best response to aging is not to cut benefits but to extend active lives. Remaining active — working, volunteering, caregiving — improves physical and mental health, reduces chronic-disease burden and allows more people to contribute to society for longer. Turning longevity into an economic and social asset requires precisely this: better health, greater participation and more opportunity across all life stages.
Technology, when applied effectively, can accelerate this shift. Assistive robots may still face skepticism, but other digital solutions are already delivering results. In Singapore, the LumiHealth program, developed with Apple, uses gamification to promote physical activity and prevention at scale. In South Africa, Discovery Health has shown that behavioral incentives can improve the health of millions while reducing system costs. These examples prove that a proactive, data-driven approach is not only feasible but effective.
Yet no innovation succeeds in isolation. It requires institutional frameworks that support cross-sector coordination, incentives that reward value rather than volume, and systems that recognize that longer lives must be matched with longer opportunities. That is the true dividend of longevity: transforming a demographic challenge into a socioeconomic strategy that benefits every generation.
MORE INFO:
“Pushing back against private practice: the unintended effects of paying public doctors more” by Jonathan Gruber, Nuria Mas, Judit Vall Castello and Jaume Vives-i-Bastida. National Bureau of Economic Research (2025).
WATCH: In this IESEconomics video, “Global health in transformation,” Nuria Mas highlights the importance of a well-functioning healthcare system, especially in the wake of the pandemic, and explains her model to improve strained healthcare systems for the sake of future generations.
This article is included in IESE Business School Insight online magazine No. 171 (Jan.-April 2026).
READ ALSO:
The future of healthcare: 5 challenges for 2030
Transforming health: how a researcher, an entrepreneur and an investor are making a difference
Check these vital signs before innovating
15% off with the code INSIGHT15
